Palliative care support is not just for patients with incurable disease. But too many providers, patients, and the general population conflate a referral to palliative medicine with impending death. And because of this, patients are often not referred to us until or unless they are imminently dying.
This frustrates the palliative medicine community because of our belief (and this is supported by well-designed studies) that a significant number of patients with complicated illnesses could benefit from our input. And this includes those patients who still have curative options!
to illustrate: A recent breast cancer tumor board experience.
Our breast cancer tumor board is typical of most around the country. It is a multidisciplinary meeting that includes a wide variety of providers who work with patients with breast cancer: oncologists, mammographers, pathologists, radiation oncologists, surgeons, plastic surgeons, nurse navigators, and a variety of cancer resource ancillary staff. And at our institution, a representative from palliative care is often there too!
Today Mrs O was discussed. She is 55 yr old, with stage iii breast cancer and has just completed neoadjuvant chemotherapy with an excellent response. Now she’s making plans for surgery. No matter what her operation (mastectomy or lumpectomy with radiotherapy), the oncologists expect that she has many years of active life ahead of her. During the presentation today- it was mentioned that Mrs O is having a hard time deciding between breast conservation vs mastectomy +reconstruction. In addition, they noted she has 2 adolescent children, a busy job, and is struggling to deal with it all. And, she continues to have side effects from the chemotherapy. From what everyone says, she sounds a bit overwhelmed.
The room got quite, so I mentioned that quite likely she could benefit from being referred to our out-patient palliative medicine clinic…
the response
The response from the physicians in the room would have been funny except that it wasn’t. They pretty much immediately (almost like a reflex) straightened up in their chairs and in unison declared “she’s not dying!”. As if that would be the only reason to be seen in our clinic…
as the Apollo 13 astronauts reportedly said, “Houston we have a problem”..
and maybe we are partially to blame…
A good picture can tell a thousand words
In the beginning:
This early model of how palliative medicine can be viewed within the confines of patient care is quite limited with concrete borders. So per this diagram, at first all treatments are meant to prolong life/cure the disease. When this approach abruptly ends, due to continued disease progression and/or lack of effective curative options, then palliative care comes in and is a completely separate plan of care until death.
The problem with this diagram is that it makes it look like an “either, or” situation. This is simplistic and wrong because providers are always providing symptom relief during curative interventions, it’s just not the main thrust of treatment.
a more recent modification
This newer diagram illustrates how palliative care can be provided concurrently with those treatments meant to cure/prolong life And as the disease progresses or as fewer disease specific treatment options are available, input from the palliative side of things increases to optimize quality of life.
However, as you can see, there remains essentially one endpoint: death and bereavement support for family left behind.
So although this newer model promotes earlier input of palliative medicine providers, is there any wonder that many equate palliative care with end of life care? There’s only one way out for these patients, and that is death.
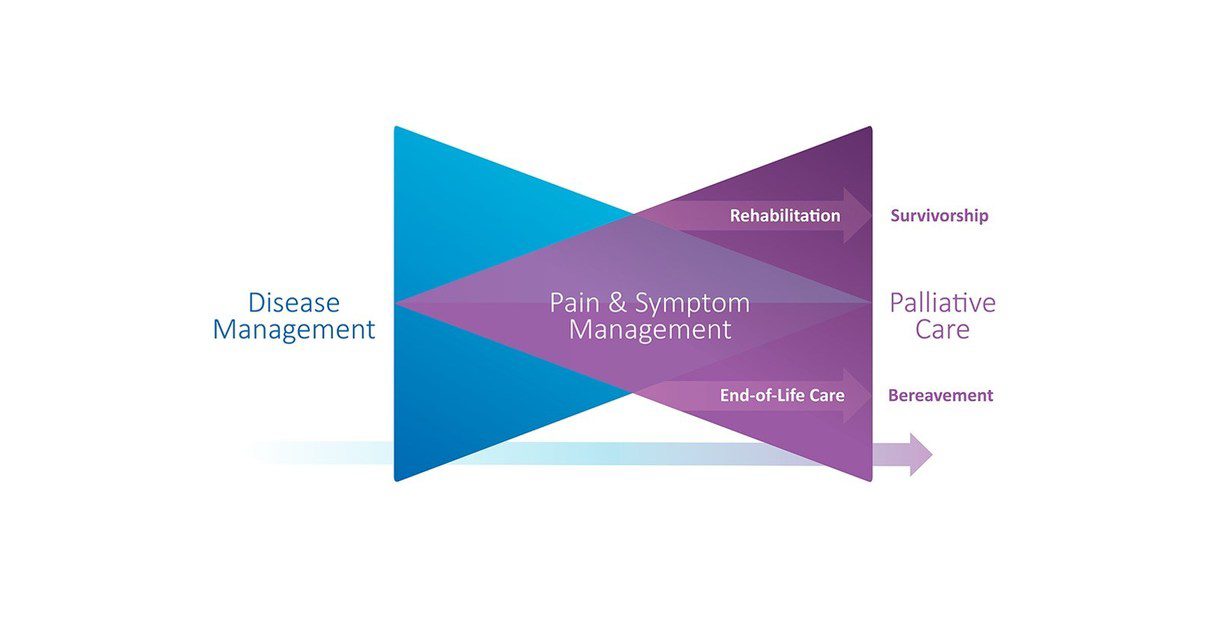
enter the Bow Tie
But there is another way. Dr Pippa Hawley from the University of British Columbia has a designed a new communication tool, to help visualize how palliative medicine can be incorporated into the care of patients with a wide variety of complicated conditions- including those that can be cured.
With this depiction, the palliative part of the overall care is in the purple. As you can see, death is not the only endpoint. Rehabilitation/survivorship is also a possibility. To quote Dr Hawley, “it is just to show and reassure patients (and I would add providers) that these services (rehabilitation/survivorship) are not excluded as possible components of their care in the future.”
So this demonstrates why patients like Mrs O who is struggling with decision making, and struggling with symptoms, and struggling with dealing with her cancer could potentially benefit from our services. Plus it removes the stigmata of ‘death’ as being sole endpoint of patients with whom we are involved. It is a much better descriptor of what palliative care services offer- and perhaps can make providers and patients more open to referrals.
Which is exactly what a good communication tool should do.
read this on Facebook too! click here



Subscribe to my blog feed